
“The Signal” is a quarterly publication that is publicly available with archived editions available to SAA Members. If you have information or suggestions for the newsletter, please send an email to SAA Communications Committee Chair – R. Ross MacLean at ross[dot]maclean[at]yale[dot]edu.
Follow us on BlueSky ![]() @ambulatory-assessment.org
@ambulatory-assessment.org
Follow us on LinkedIn ![]() https://www.linkedin.com/company/society-for-ambulatory-assessment/
https://www.linkedin.com/company/society-for-ambulatory-assessment/
Conference Information
Abstract submissions are now OPEN for the 2026 SAA Conference in Vienna!
Have some fantastic science that you want the world to see? Maybe its a new finding or method, or maybe you had some time to finally complete an analysis that has been on back burner for all of 2025. Consider submitting your work to be included in the SAA Conference in Vienna!
Professor Laura M. König and the Health Psychology Group will host the SAA 2026 conference at the Universität Wien | University of Vienna. The Local Organising Committee of the 2026 SAA conference is delighted to invite you to submit an abstract for consideration for a presentation at the Society for Ambulatory Assessment conference 2026, which will be held in Vienna, Austria, from 3rd to 5th August 2026.
1. Call for Abstracts
Submissions are invited for the following formats:
- Symposia: Consisting of 4-5 presentations focused on a particular topic, and a discussion or activity (e.g., demonstrating a tool, an algorithm or a novel approach to data analysis). Symposia will be scheduled for a total of 75 minutes. Symposia must include presenters from at least two different institutions, preferably from at least two different countries.
- Oral presentations: 10 minutes to present an empirical study, literature review or conceptual paper, followed by 2 minutes for questions from the audience. Presentations will be grouped thematically in sessions of 75 minutes length.
- Poster presentations: Posters will be grouped thematically in chaired sessions. On-site participants will be asked to briefly present their poster in approx. 3 minutes, following 2 minutes for questions from the audience.
Please also take a look at the submission guidelines on the conference website, which provide further information on the formats, including structure and word counts of the abstracts: https://univie.eventsair.com/saa2026/submission Please note that individuals can only submit ONE oral or symposium presentation and present ONE poster. Individuals can additionally be a discussant or activity coordinator in ONE symposium.
The submission deadline is 16 January, 23:59 CET.
The conference will be held as a hybrid event, allowing on-site and online participants to interact in symposia and oral sessions. Online participants will be asked to present live, in case their contribution is accepted as an oral presentation or as part of a symposium. All poster presenters will be asked to upload their posters to a secure platform that will only be shared with conference attendees. Please note that online participants whose submission was accepted as a poster will be given the opportunity to have their poster printed and displayed on-site (at a cost), but will not be able to interact with on-site participants during the poster session.
2. Keynotes
We are furthermore excited to announce our two invited keynote speakers – Professor Brenda Penninx and Professor Eiko Fried. Professor Penninx will provide insights into stress in daily life, including first insights from the Stress in Action project, which she is coordinating. Professor Fried will share pitfalls and promises of ambulatory assessment methods in mental health science to measure minds in motion, which he has gathered, amongst others, while working on his ERC Starting Grant. We are very much looking forward to both presentations! Learn more about the keynote speakers and their work on the conference website.
The third and final keynote of the conference will be delivered by the SAA Early Career Award recipient. A call for nominations will be published through the SAA communication channels shortly.
3. Stay up to date on social media
Stay up to date on conference-related announcements by following the conference accounts on Bluesky and Linkedin. Until Christmas, we have a special treat for you in our advent calendar – a beloved Austrian Christmas tradition for people of all ages – and share insights about the conference and its location every day.
SAA Spotlight
Dr. Antoinette Poulton: Challenges and benefits of assessing cognition using ambulatory assessment
For this spotlight, we spoke with Dr. Antoinette Poulton, a NHMRC MRFF Early to Mid-Career Research Fellow at the University of Melbourne in Australia. Dr. Poulton’s research focuses on executive function and transition to addiction. Dr. Poulton has developed smartphone technologies that can be used to provide real-time information about drinking, self-control and reward sensitivity, and the feasibility of collecting data in daily life. Dr. R. Ross MacLean, PhD (Communications Committee member) interviewed Dr. Poulton to learn more about naturalistic assessment of cognition using mobile devices.
Ross MacLean: Can you provide a brief overview of how you became interested in naturalistic assessment of cognition?
Antoinette Poulton: I became interested in naturalistic assessment of cognition in around 2015. I had just commenced my PhD, which was centred on impulsivity (especially choice impulsivity and response disinhibition) and vulnerability to transition from alcohol misuse to alcohol use disorder (AUD). Around the same time, I encountered a student in the secondary school boarding community where my partner worked who was teaching himself how to program apps. He was looking for a real-world project to test his skills, so we commissioned him to program our first app, Alcohol Capture. Our early work with Alcohol Capture included encouraging validity and reliability studies (Poulton et al., 2018, 2019), but, ultimately, tracking alcohol consumption in real-time did not seem to assist in clarifying the role of impulsivity in vulnerability to transition from alcohol misuse to AUD (Poulton et al., 2022).
We started to consider ways we could assess impulsivity in real-time, thinking perhaps that daily fluctuations in impulsivity might be more closely linked to real-time alcohol intake. Along with two other postgraduate students in Prof Hester’s lab (Dr Gezelle Dali and Ms Evelyn Chen), we began working on the CheckCog app. By this time, the student who had worked on Alcohol Capture had graduated university and started his own app development company (Ant Development Studios). We again worked with him, eventually programming two cognitive tasks (Stop-Signal Task and n-Back) that sit within CheckCog. Last year, we published a psychometric study, finding the tasks reliably chart within-person differences in response inhibition and working memory (Dali et al., 2024). Currently, we’re using the app in studies charting the relationship between naturalistic assessments of cognition and alcohol use, but it has also been utilised in postgraduate studies focused on mild traumatic brain injury recovery trajectories.
RM: I love to hear when seemingly random connections result in collaboration. What types of cognition are most amenable to measuring via ambulatory assessment?
AP: Over time, there have been huge advances in app capabilities so, today, there are few technological barriers to using apps to assess any type of cognition. Advances in software and hardware synchronisation have now largely overcome concerns about the precise presentation of stimuli and the accurate recording of response time.
In general, processes that can be captured reliably in short, repeatable, low-burden tasks are most amenable to ambulatory assessment. Core executive and attentional processes – such as working memory, inhibitory control, cognitive flexibility, sustained and selective attention, and processing speed – are particularly well suited, as they fluctuate over short timeframes and can be measured using brief, abridged versions of standard paradigms. These domains are sensitive to contextual influences such as stress, fatigue, mood, and substance use, providing rich within-person data on cognitive variability in daily life. Decision-making processes, such as those related to probabilistic learning, temporal discounting, and risk-taking, have all also been successfully adapted for ambulatory assessment. By contrast, tasks assessing complex reasoning or language-based functions are less suitable for ambulatory assessment due to participant burden, practice effects, and greater susceptibility to disengagement and cheating.
RM: What are the biggest challenges to measuring cognition in the context of daily life?
AP: We have faced a few challenges over the years. Unlike a controlled lab setting, we have no control or even knowledge around what else might be going on when participants do the task. As much as we can direct participants to do tasks in quiet locations, when we’re asking them to do them multiple times a day, all manner of distractions might be impacting performance. In the case of timing-based tasks, such as the Stop-Signal Task, performance could be impacted by, for instance, a television on in the background or a conversation unfolding nearby. Memory-orientated tasks, like the n-Back, might be susceptible to cheating, with participants potentially making notes as they work through trials. Equally, we don’t know whether participants might be seated in such a way that performance is hindered or whether they have sufficient light to properly see stimuli or at what volume they have set their device. While some of these issues are perhaps less problematic for within-person studies, they do nonetheless contribute to noisy data.
There are also challenges around compliance. Naturalistic data is appealing because we can assess participants daily, or even multiple times a day. This can, however, constitute a heavy burden for participants. We often find they submit data less often or for a shorter period than we had hoped. Balancing burden against the advantage of multiple assessments can be tricky. I have found that, over time, compliance has dropped in studies reliant on ambulatory assessment. I have wondered whether this might be related to high saturation with apps generally. We now use a multitude of apps in daily life. Being asked to use an app to track cognition is therefore possibly no longer the novelty it might once have been.
An ongoing challenge relates to the software itself. Collaborating with software developers takes time, and building an app sophisticated enough to capture timing and accuracy while incorporating a secure backend database can be costly. Ethics requirements around data collection and management procedures can add to this cost, depending on the level of security needed. Aside from initial expenditure, operating systems and devices constantly change. As such, there is an almost continuous need to upgrade native mobile apps. This is again costly and can interrupt data collection. Over time, the backend can become completely outdated and a major re-build is necessitated.
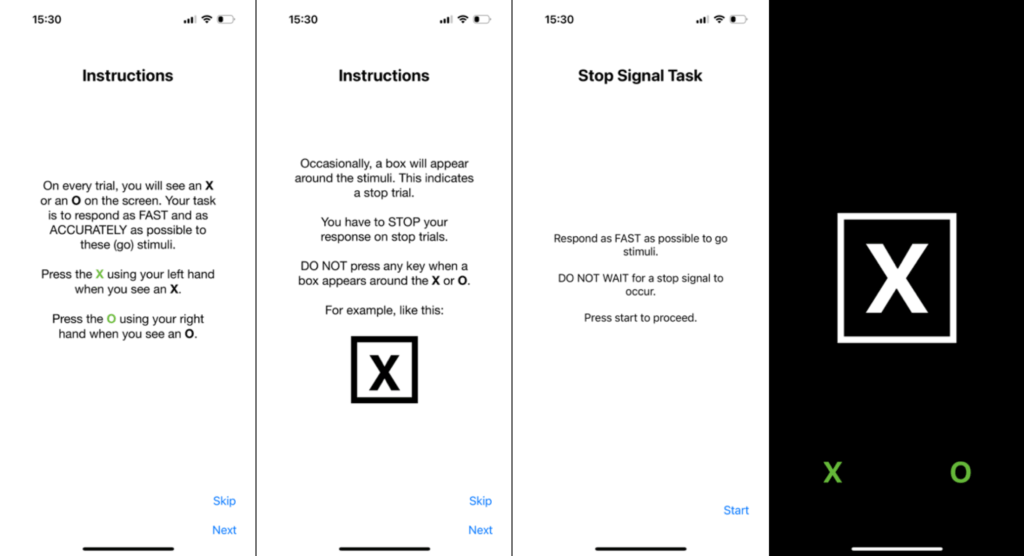
Above: Screen grabs from the CheckCog stop-signal task
RM: These challenges sound all too familiar. I imagine distraction is more of a concern when attention to stimuli is imperative to the construct being measured. What are the advantages of naturalistic cognitive assessments?
AP: Naturalistic cognitive assessment overcomes some of the disadvantages associated with traditional laboratory-based cognitive assessment. Task performance in controlled laboratory environment is unlikely to accurately reflect how we might perform the task in the real world, where our cognition is impacted by fluctuating internal emotions and variations in our external environmental. Indeed, a growing body of work demonstrates associations between variations in cognition, internal states, and external conditions. Naturalistic cognitive assessment thus provides greater insight into the dynamic relationships between daily life factors and cognitive function. So, as much as the uncontrolled environment might be seen as a challenge, naturalistic cognitive assessments offer insight into authentic cognitive ability in realistic settings.
This type of assessment also enables researchers to investigate within-individual dynamics, such as tracking the trajectory of cognitive changes associated with traumatic brain injury, drug and alcohol use, and other disease. Moreover, as naturalistic cognitive assessment allows repeated assessment, cognition in this context can be measured in concert with other factors, such as mood, fatigue, sleep, stress, and drug/alcohol intake. Because of its temporal granularity, this type of assessment can detect subtle cognitive shifts preceding clinical or behavioural changes. A complex picture can thus emerge regarding the constellation of factors involved over the course of various conditions and diseases. In turn, the individualised nature of the data facilitates personalised intervention and/or feedback plus monitoring of real-time treatment response.
A further advantage relates to enhanced sample size and diversity. Naturalistic cognitive assessments electronically are highly accessible. In Australia, where we have a small but substantial proportion of the population living in rural and remote locations, this means we can conduct studies that include people who reside thousands of kilometres from any research institution. It also means we can more easily include persons traditionally under-represented in cognitive research, such as those with physical disabilities, pregnant persons, or older individuals. In this way, samples from studies utilising naturalistic cognitive assessments are richer and might better represent the general population.
RM: Accessibility can be such an important advantage of mobile assessment to include individuals who otherwise would be unable to participate. As you have developed ways to evaluate cognition using mobile assessments, what have been some things that surprised you?
AP: I am still surprised that so few researchers are assessing cognition in real-time. There seems to be an abundance of studies using apps to measure affective and emotional states, motivation, behaviour, physical and psychiatric symptoms, and contextual factors, yet relatively few target cognition. This likely reflects the complexity of programming cognitive tasks and the initial financial outlay required, but it remains surprising. Additionally, few of these studies reported detailed psychometric evaluation or provided data on compliance and reactivity, suggesting the field is still maturing and ripe for further activity.
I also marvel at just how variable cognition is within individuals across short timescales. Early on, I expected daily fluctuations to be relatively modest, but repeated assessments have revealed striking within-person variability in our work on response inhibition and working memory. This reinforces the idea that cognitive performance is strongly influenced by contextual factors such as sleep, fatigue, mood, and stress. Taken together, these findings suggest that isolated, one-off measures of cognition may tell us relatively little. When cognitive performance is assessed in context and examined alongside other fluctuating states, the resulting data provide a far richer and more ecologically valid picture of how people think and function in everyday life.
RM: How do you imagine the ways ambulatory assessment of cognition will be used 5 to 10 years from now?
AP: I would expect ambulatory assessment of cognition will be deeply integrated into both research and clinical care. Cognitive testing will move beyond the laboratory and become a core component of digital phenotyping. By incorporating ongoing real-time assessment of cognition, researchers and clinicians will more fully be able to model cognition as a dynamic process, continuously shaped by individual and environmental variables.
I anticipate the use of more sophisticated adaptive algorithms that tailor task difficulty based on prior performance, enabling both fine-grained within-person tracking and highly individualised baselines. These data will support early detection of cognitive decline, relapse, or recovery trajectories across conditions ranging from addiction and mood disorders to concussion and neurodegenerative disease.
Integration with smartphones and wearables will make cognitive monitoring passive and continuous, blurring the line between assessment and intervention. For example, subtle declines in inhibitory control might automatically trigger cognitive-training prompts or real-time behavioural feedback.
Finally, I think we’ll see a shift toward participatory models of cognitive assessment, where participants access their own cognitive data and use it for self-reflection or goal-setting. In this sense, ambulatory cognitive assessment will evolve from a research tool into a personalised health technology, supporting prevention, rehabilitation, and everyday cognitive wellbeing.
RM: Sounds like we have a lot to look forward to. Thank you for your time!
Research Brief
This month, Dr. Haijing Hallenbeck (SAA Committee Member) reached out to Dr. Björn Siepe to discuss his recently published manuscript in Journal of Psychopathology and Clinical Science entitled “Associations between ecological momentary assessment and passive sensor data in a large student sample.” This publication used data from the WARN-D study, which is a 5-year project led by Dr. Eiko Fried at Leiden University. The project collects smartwatches and smartphone data from 2,000 students living in the Netherlands over two years. The manuscript led by Dr. Siepe examined the concordance between self-reported and passive data in the measurement of stress, tiredness, and sleep.
Haijing Hallenbeck: What was the inspiration behind the paper?
Björn Siepe: Millions of people use smartwatches daily to monitor stress, sleep, and activity, but how well do these devices actually capture what we’re experiencing? In clinical psychology research, combining self-reported experiences with passive sensor data has become increasingly popular, but we still don’t fully understand how well these different data sources actually overlap. The smartwatch we used in the WARN-D project doesn’t just track basic metrics like steps or heart rate; it also provides inferred measures like ‘stress levels’ that millions of users rely on daily. Given how widely these features are used, both in research and everyday life, it’s crucial to validate whether they actually measure what we think they do.
Above: Members of the WARN-D team
HH: What was the process like working on this project?
BS: We came up with the idea for this project when we started plotting some of the data and found some surprising patterns. For example, the self-reported and physiological distributions looked very different. This sparked our interest in investigating this further to improve our understanding of both self-report and passive sensing data. One of the struggles that we faced during this investigation was the large extent of researchers’ degrees of freedom when working with sensor data, as they can be aggregated and summarized in many different ways. We therefore choose a larger grid of sensitivity analyses to ensure that results aren’t tainted by arbitrary decisions in the modelling pipeline.
HH: How did writing this paper shape your thinking on this topic?
BS: This project has made me both more curious about passive sensing data and more critical of its use in research. While I can see that information about general physical activity or sleep duration could be useful for understanding and predicting mental health, I’m unsure how well passive sensors can capture more abstract concepts, such as stress or tiredness, accurately. While reading the literature, I came across the idea of a potential ‘semantic gap’ between passive and self-report data. This means that users may understand stress differently from how the smartwatch interprets it. It is useful to understand that smartwatches may not be able to replace self-reporting, but may be able to augment it in some cases. Given that commercial-grade smartwatches provide direct feedback to millions of people worldwide, essentially constituting a large-scale intervention, I would also be interested to know how this feedback affects users positively or negatively.
HH: What advice do you have for a student or researcher that is considering a project that integrates passive data collection with EMA?
BS: There are many things to consider, but luckily, there is now useful literature on the subject (e.g. Velozo et al., 2024, https://doi.org/10.1017/s0033291722002367). One specific piece of advice that I would give after finishing this project is to check the overlap between passive sensor and self-report data. Even if you’re mainly interested in prediction, understanding this relationship will help you interpret your results and avoid misleading claims.
HH: As mentioned in the paper, sensor data has a high frequency sampling than EMA reports, which necessitates aggregation of data. How did you decide to aggregate the sensor data?
BS: In the absence of clear guidelines or theoretical expectations, we used a grid of aggregation windows (ranging from 15 to 240 minutes) and time frames (aggregation before, during, or after the EMA prompt). Additionally, we used the mean, the standard deviation, and the maximum of the sensor data as aggregation statistics. Overall, these choices did not have a strong impact on our results, making us more confident in their robustness across plausible alternative specifications.
HH: In your study, momentary self-reported stress was assessed four times per day for over 85 days. How could passive data be integrated into other mobile survey methods, such as event surveys where a participant initiates a survey during times of subjective stress?
BS: One of the strengths of passive data is their continuous assessment, so it would be relatively straightforward to combine them with irregularly timed event surveys. It would be interesting to see if associations between passive and self-report data would be stronger for such types of surveys.
Thank you Dr. Siepe for taking time to discuss your exciting work. The manuscript can be accessed here. For more information about the WARN-D study and additional research, check out the lab website at: https://warn-d.eiko-fried.com/
Opportunities and Education
Get involved in the SAA Executive Committee!
Every other year, four or five members of the Executive Committee are rotating off. Next year, five positions on the Executive Board will be vacated and we are looking for candidates for the following positions:
President-Elect (2026 – 2028; to become President 2028 – 2030)
Treasurer (2026 – 2030)
Member-at-Large (2026 – 2030)
Early Career Member-at-Large (2026 – 2028)
Are you interested in running for one of these four positions? Or would you like to nominate a colleague? Then please send an email to us ([email protected]).
All regular members are eligible for running for the positions of President-Elect, Secretary, and Member-at-Large. Early career members and regular members who are currently pursuing their degree (MSc, PhD or similar) or who have obtained their doctoral degree in 2024 or later are eligible for the position as Early Career Member-at-Large.
Elections for these four positions will be held in early 2026. If you have any questions about these positions or the nominating process, please do not hesitate to contact the current members of the Executive Committee or the Chair of the Nominating Committee:
Ulrich Reininghaus: Ulrich[dot]Reininghaus[at]zi-mannheim[dot]de
Notifications and Recognition
Professor Inez Myin-Germeys Awarded Honorary Doctorate by University of Basel
On November 28, 2025, Professor Inez Myin-Germeys received an honorary doctorate from the University of Basel, in recognition of her groundbreaking work in mental health research. The University of Basel praises her exceptional and pioneering contributions to our understanding of how moment-to-moment environmental and social stressors influence the onset and progression of psychiatric symptoms.
The University of Basel, one of Europe’s oldest and most prestigious universities, awards honorary doctorates to scholars who have made exceptional contributions to science and society. This honor reflects its commitment to advancing research that impacts global mental health.
This distinction celebrates:
- Her pioneering role in using the Experience Sampling Method (ESM) to study mental health in real-life contexts.
- Her emphasis on the role of context in psychopathology, reshaping theory and clinical practice.
- Her leadership in digital mental health, a rapidly growing field bridging science and care.
“I am deeply honoured by this recognition,” said Professor Myin-Germeys. “It reflects the importance of studying mental health in daily life and the potential of digital tools to personalise care.”
Professor Myin-Germeys is based at KU Leuven, where she heads the Center for Contextual Psychiatry, and leads IMMERSE, a major European initiative advancing digital mobile mental health tools. Her research continues to shape the future of personalised, context-aware mental health care.
On behalf of the SAA Communications Committee, congratulations Prof. Myin-Germeys!
Community Information
SAA is now on LinkedIn!
We are now on LinkedIn! One of the goals of the Communications Committee is to build a sense of community for our members. We hope to use our page on LinkedIn as a place for members to share news about published manuscripts, job opportunities, and general announcements that may be relevant for other SAA members. Click here to follow our page. To help build our community, please invite your LinkedIn connections to also follow our page.
Renew your SAA Membership for 2026 today!
Now is the perfect time to renew your SAA membership for the coming year to get the most out of your membership benefits including:
- Reduced registration fees for the SAA Annual Conference and SAA-initiated Workshops, which includes presentations of new theory, methods and research in the form of invited addresses, symposia, poster sessions and Presidential and Award addresses.
- A Membership Directory with contact information of all members, along with dates and locations of future conferences and access to the Officers and Executive Board.
- Periodic mailings about SAA and other ambulatory assessment related events and opportunities.
- A developing awards program
- Access to archived editions of The Signal
Visit https://ambulatory-assessment.org/ and (1) log in to your account (top right corner), then (2) go to Membership “Apply for / Renew membership” and click on “Click HERE To Apply for or Renew your SAA Membership“.
Regular members:
- Click on the Application button next to Regular – RENEWAL
- On the next screen, please review your account information and update the information if applicable. Click on Continue Application.
- You are then being forwarded to PayPal. You can purchase the 2026 membership either by logging into your PayPal account or pay by Debit or Credit Card.
Early career members:
If you currently are in an undergraduate, graduate, or pre-doctoral training program or within three years after attaining their doctoral degree (i.e. you obtained you doctoral degree in 2023 or later), you qualify for an Early Career membership at a reduced rate of 45€ (vs. 95€ for regular membership).
- Click on the Application button next to Early Career
- On the next screen, please review your account information and update the information if applicable.
- Upload a current CV and a document verifying your status as an early career researcher (e.g., certificate of enrollment, diploma). Alternatively, you can also upload a short note from a current SAA member supporting your application (This is not required. A CV and document verifying your status as an early career researcher are sufficient).
- Click on Continue Application.
- You are then being forwarded to PayPal. You can purchase your 2026 membership either by logging into your PayPal account or pay by Debit or Credit Card
You are not a current member and would like to purchase a 2026 membership?
In this case, please visit https://ambulatory-assessment.org/membership-level-selection/, select the appropriate level of membership (Regular – NEW or Early Career) and follow the same steps as described above.
After completing these steps you will receive an automated e-mail from PayPal with a payment receipt. After we have finished processing your order, you will receive an additional receipt from us ([email protected]). Please note that this may take up to 5 business days.
In case you encounter any problems with purchasing your memberships, please contact us ([email protected]). We are looking forward to receiving your membership renewals and hope that you will continue to be a part of this society!
SAA Communication Committee Members
- R. Ross MacLean, Ph.D. (Committee Chair), Yale School of Medicine and VA Connecticut Healthcare System
- Lauren DiPaolo, Ph.D., Corporal Michael J. Crescenz VA Medical Center
- Anne Grünert, Ph.D., RWTH Aachen University
- Haijing Hallenbeck, Ph.D., VA National Center for PTSD and Stanford University Medical Center
- Laura König, Ph.D., University of Vienna
- Femke Lamers, Ph.D., Amsterdam University Medical Center