
“The Signal” is a quarterly publication that is publicly available with archived editions available to SAA Members. If you have information or suggestions for the newsletter, please send an email to SAA Communications Committee Chair – R. Ross MacLean at ross[dot]maclean[at]yale[dot]edu.
Follow us on BlueSky ![]() @ambulatory-assessment.org
@ambulatory-assessment.org
Join us on LinkedIn ![]() https://www.linkedin.com/company/society-for-ambulatory-assessment/
https://www.linkedin.com/company/society-for-ambulatory-assessment/
Conference Information
SAA 2026 Conference: 3 – 5 August 2026
In just a few months, the SAA 2026 Conference will take place at the University of Vienna in Vienna, Austria. The conference will be hosted by Prof. Laura König and her team at the Health Psychology Lab and the EMA Lab.
The University of Vienna is set in the heart of one of Europe’s most beautiful and historically rich cities. With its impressive architecture, central location, and close proximity to many of Vienna’s cultural landmarks, the University’s Main Building offers a truly special setting for the conference. Attendees will also have the opportunity to experience Vienna itself, with its historic streets and vibrant cafés.
Interest in SAA 2026 is already exceptionally strong, with over 400 attendees registered so far, which reflects the growing excitement surrounding the event. The Organising Committee is dedicated to preparing what promises to be one of the largest and most engaging SAA conferences to date.
The detailed scientific programme will be published on the conference website (https://univie.eventsair.com/saa2026/) in the coming weeks. Alongside a diverse programme of talks, symposia, posters and workshops, the Organising Committee is also placing a strong emphasis on opportunities for networking.
Planned networking opportunities include a treasure hunt through Vienna followed by informal drinks for Early Career Researchers, a networking reception in the historic courtyard of the University of Vienna, and a conference dinner at Vienna’s oldest Heuriger, where the Mayor of Vienna, Michael Ludwig, will also be in attendance. In addition, the SAA Mentoring Lunch will provide a dedicated opportunity for mentees and mentors to meet, connect, and exchange experiences. We are excited for our two keynote speakers (Prof. Brenda Penninx and Prof. Eiko Fried) who will be joined by the SAA Early Career Award winner (TBA)!
The networking reception is included in the conference ticket. Dinner tickets and spaces for the mentoring lunch – especially for mentors – are still available and can be booked via the conference registration platform: https://univie.eventsair.com/saa2026/regregularen/Site/Register
To help attendees make the most of their stay, the team will also publish helpful guides for visiting Vienna. These will include practical recommendations, cultural highlights, and local tips to support participants in exploring the city before, during, and after the conference. We will also set up a Whatsapp group for participants to informally connect between and after sessions.

SAA 2026 promises to be an inspiring, lively, and memorable conference!
SAA Spotlight
A discussion with Dr. Nicholas Jacobson on the present and future of passive data collection
For the summer spotlight, R. Ross MacLean, PhD (Communication Committee Chair) connected with Nicholas Jacobson, PhD to discuss passive data collection. Dr. Jacobson is a researcher and Associate Professor at Dartmouth College in the United States. His research (AIM HIGH laboratory) is focused on using multimethod assessment utilizing passive sensor data from smartphones and wearable devices to enhance the assessment and treatment of anxiety and depression.

R. Ross MacLean: For those that may be new to passive data collection in the larger field of intensive longitudinal designs, how would you define constructs or variables as passively recorded?
Nicholas Jacobson: A passively recorded variable is one we capture without asking the participant to do anything in the moment. The sensors on phones and wearables run in the background, and we derive constructs from that stream afterward. Step counts, sleep duration, time on screen, GPS-based mobility, heart rate, and heart rate variability are typical examples. The contrast is active EMA, where the participant must pause to answer a prompt. Passive data is the layer that keeps recording even while the person is asleep or otherwise engaged.
RM: As a bit of an introduction to your work, how did you get involved in passive data collection and what types of passive data streams do you most commonly work with?
NJ: I have a software development background, and I started building apps in grad school. I built my first sensing system in the summer of 2012, mostly because I wanted to test whether the signals coming off a phone could pick up on day-to-day mood. From there I kept building, and the streams kept expanding. Most of my current work falls into two buckets. The first is smartphone data, things like GPS, accelerometry, screen state, app and communication metadata, and ambient light. The second is wearable data, primarily actigraphy, heart rate, heart rate variability, and sleep. We also pull in audio-derived features depending on the protocol.
RM: That is quite an arsenal of data. How do you decide when passive sensing is preferable to active EMA prompts, and when you combine them?
NJ: My rough rule is that passive is better when the construct is observable behavior, and EMA is better when the construct lives inside someone’s head. Screen time is a good example. If I want to know how long someone is on their phone, the passive estimate will beat self-report every time, because people are not great at retrospectively quantifying that. The same goes for sleep, mobility, and physical activity. EMA, on the other hand, is hard to beat for internal states like anxious thoughts, urges, mood quality, or perceived stress. You can sometimes proxy those passively, but you are usually doing it indirectly. We often combine the two because the most interesting questions tend to be about how behavior and experience relate, and you need both sides to model that.
RM: How do you handle data missingness or device data drop out in real-world passive sensing studies?

NJ: Missing data is one of the hardest parts of this work, and it never fully goes away. We rely on the usual model-based approaches, including multiple imputation and full information maximum likelihood, alongside masking layers inside deep learning models that let the network reason about which inputs are present at a given time. None of those are silver bullets, and we are still actively developing new methods. One of my students have made missing data in intensive longitudinal designs their primary focus, because the temporal structure makes a lot of standard techniques less appropriate than people often assume.
RM: How has the increased ownership and familiarity with wearable technology changed what’s feasible in intensive longitudinal design research?
NJ: It has changed a lot in the last decade. When I started, asking a participant to wear a device for a few weeks was a real ask. Now people often come into a study already wearing one, and they think nothing of charging it overnight. That has made bring your own device designs much more realistic, and it has stretched the feasible study duration from weeks to months, and in some cases years. It also lowers reactivity, because the device is part of their routine before we ever show up.
RM: How do participants typically respond to passive monitoring, does it affect behavior or dropout rates?
NJ: Most participants adjust quickly, and within a few days the monitoring tends to fade into the background. The reactivity we see is usually smaller than what we see from active EMA, because there is no recurring prompt to remind them that they are in a study. Dropout is driven much more by EMA burden and technical friction, like battery drain or app crashes, rather than any discomfort with the passive piece.
RM: What are the ethical considerations when developing or recording passive variables in the context of someone’s daily life?
NJ: This is something I have spent a lot of time on, and I co-authored a paper laying out the considerations in more depth. The short version is that meaningful consent is harder than people often appreciate, because participants need to understand both the surface-level recordings and the deeper inferences we can draw from them. Location data and communication metadata are particularly sensitive, and the inferences we can draw from them go well beyond what was on the consent form unless you write it carefully. Other big areas include downstream data control and the equity issues surrounding who actually owns high-quality devices.
RM: What are the most common misinterpretations you see when researchers use passive data without sufficient expertise?
NJ: The most common one I see is people underestimating how much data they are actually losing. Keeping a sensing app running reliably on a participant phone is much harder than it sounds (in many ways we act in ways that the operating systems don’t want us to). A lot of teams report data completeness numbers that quietly assume the app was running when it was not. The second is on the processing side, where small data-cleaning and feature-extraction choices can drastically shift downstream results. The third is around machine learning framing. There is a real difference between detecting a current state versus forecasting future risk. People sometimes throw all of those into the same modeling pipeline without thinking carefully about which one is actually clinically useful.
RM: What can passive data not tell us that people sometimes assume it can?
NJ: It cannot tell you the why. We might know a participant barely slept and stayed home all day, but sensors alone won’t reveal if they were battling a depressive episode or just recovering from the flu. The internal experience, and the meaning a behavior carries for a person, are not in the data. People also sometimes treat passive data as causal evidence, and it almost never is on its own. Most of what we publish is correlational structure across very rich, very autocorrelated signals.
RM: Where do you see passive data collection heading in the next 5 to 10 years?
NJ: The direction I am most excited about is tighter integration of sensing and intervention. I think we are going to see a lot more just in time adaptive interventions powered by smarter inferences from passive data, and recent progress in foundation models gives us the opportunity to make those decisions more individualized and more context aware than the rule based approaches of the last decade. We are working on this in the lab right now, and the early results are very promising.
RM: Are there populations or conditions where you think passive data collection could be transformative but hasn’t been tried yet?
NJ: Functional behavior in a range of health conditions is hugely underutilized. We tend to focus on psychiatric phenotyping, but there are large populations where day to day functioning matters more than any single symptom rating, including chronic pain, neurological conditions, severe mental illness, and recovery from surgical or oncologic care. Passive sensing is a natural fit there, because functioning unfolds outside the clinic and we have very limited tools to measure it. I would expect this to be one of the bigger growth areas over the next decade.
RM: Thanks for your time. It will be exciting to see new methods develop from advances in research and technology.
Research Brief
This past month Lauren DiPaolo, PhD (Communications Committee member) interviewed Drs. Robert Edgren, Dario Baretta, and Jennifer Inauen about their article in Communications Psychology titled “Habit degradation strategies promote faster early reductions in unhealthy snacking habit strength in intensive longitudinal randomised controlled trial.” The study is a brilliant and novel example of combining randomised controlled trials with intensive longitudinal designs and helps to bring experimental methodology to real-world settings. The trial tested the efficacy of three habit degradation strategies and the use of reward for decreasing unhealthy snacking habits. Participants completed self-report assessments via smartphone over 13 weeks. While results showed that unhealthy snacking habits declined across all groups, steeper reductions in week 1 were observed for the intervention groups compared to the control condition. The full article is available open access here. We are excited to share the team’s insights on their work and hopes for future research in this area. Responses below are identified with initials; responses with “ALL” reflect a collaborative response from the authors.
Lauren DiPaolo: What inspired you to study habit degradation?
Robert Edgren: Addiction and risk-behaviour change were core research interests for me from early on, which led me to study gambling problems. Researching habit degradation was the culmination of this passion, combined with the opportunity to pursue it as a PhD within the HABIRUPT project established by Dr. Jennifer Inauen.
Jennifer Inauen: I’ve long been fascinated by the topic of habit as a psychological concept that is fundamental to human nature, and that is not inherently “good” or “bad”. Focusing on habit degradation was motivated by our group’s focus to understand and promote long-lasting behavior change (behavioral maintenance). Dormant habits (habits that are still present in the mind, even though the behavior is no longer performed) can be a barrier to behavioral maintenance, because people can fall back into these habits when their self-regulatory resources are low. Therefore, we aimed at finding ways of degrading such habits.
LP: Which habit degradation strategy is your favourite?
RE: At the root of any approach to habit degradation lies inhibition, which is why I would consider it the most fundamental strategy. That said, in terms of providing an actionable solution for degrading a habit, I personally find substitution to be the most helpful. For example, the habit of eating a chocolate bar during an afternoon break can be substituted with a healthier alternative (which simultaneously requires wilfully abstaining from eating chocolate in the moment, i.e. inhibiting the unwanted habitual response).
JI: At the beginning of this study, I was not partial to any particular habit degradation strategy. Our aim was to determine, which one is the most effective. However, we learned through a qualitative follow-up study to our RCT that people routinely combined multiple habit degradation strategies, even in the control group, where they were not exposed to them by our intervention. This makes me think that favouring any one strategy over the other might not be helpful, as they might best work in concert.
Study authors Robert Edgren (left), Dario Baretta (center) & Jennifer Inauen (right)
LP: What was the process like to utilize naturalistic intensive longitudinal methods to study processes often examined experimentally in a laboratory setting?
ALL: A great deal of planning and piloting went into establishing the study design and developing the interventions.
There is a wealth of prior research investigating habit-related processes in daily life, so there were ample resources to draw from. That said, interventions always require contextualizing to the target behaviour and population. For example, we did a pilot study where participants rated the reward messages in terms of the rewarding nature of those messages. This preparatory work needs a lot of care and time.
One important lesson from this study concerned intervention fidelity. Many participants did not adhere to their assigned habit degradation strategy and instead adaptively blended several strategies. Coming to terms with the extent of this was something of an awakening, partially facilitated by qualitative follow-up interviews we conducted with selected participants. Hearing participants describe their experiences made clear that the gap between our experimental intentions and their lived reality was at times substantial. We are currently preparing a manuscript reporting these qualitative findings, which we intend to share later this year.
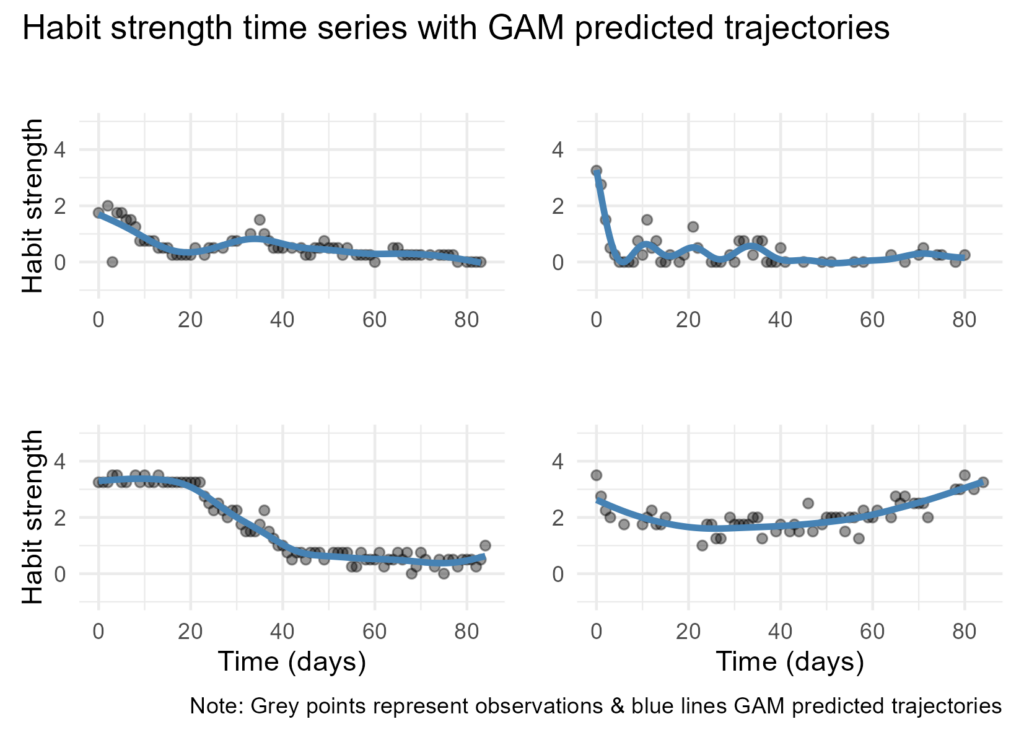
Example time series of habit strength using generalised additive models (GAM)
LP: What advice would you give to other researchers who are considering using an experimental intensive longitudinal study design to maximize ecological validity?
RE: Researchers should be mindful of how participants may experience changing demands in daily life and adaptively pursue their goals. For instance, providing written instructions to use a particular behaviour change technique offers no guarantee that other techniques will not also be used. Researchers should strive to leverage naturally occurring constraints that help avoid contamination of experimental conditions (e.g. controlling the availability of snacks at various workplaces), and where this is not possible, include ways of detecting such contamination (e.g. requesting participants to keep log of strategies used).
LP: How do the results of this paper shape your thinking about how to meaningfully capture change in habit over time?
RE: In terms of measuring change over time, I am a big fan of using generalised additive models on account of their flexibility and suitability for capturing non-linear processes. Importantly though, measuring habit accurately is a prerequisite for capturing meaningful change. Indeed, how habit strength can and should be measured in daily life contexts has been a recurring discussion topic in habit research—and to be honest, a consistent source of headache. At this point, my two cents are that habit strength can only be measured indirectly (e.g., inferred from self-report or behaviour), and for that reason it would be preferable to use multiple different types of measurement instruments. This would hopefully provide greater confidence in results through convergent validity.
JI: Indeed, measuring habit in daily life is very difficult. Currently, in daily life research, habit is mostly assessed using questionnaires (predominantly the Self-Report Behavioural Automaticity Index by Gardner et al., 2012). However, this is not ideal as we’re trying to capture an implicit concept using explicit measures. We’re currently conducting a scoping review of habit studies, including neuropsychological laboratory studies to see if there are better ways to measure habit in daily life.
LP: What do you see as the most important next steps for this research?
ALL: For habit research, important next steps include improving measurement as noted above, as well as establishing the role of single cue-behaviour pairings underlying a habit in facilitating broader behaviour change for various behaviours. For instance, a medication-taking habit may facilitate all the behaviour change required in a given context, while breaking an individual smoking-related habit may only account for a small proportion of an individual’s overall smoking. It seems we at times take the inherent value of making and breaking habits for granted, when arguably this should be established more thoroughly through empirical work.
Education and Membership Opportunities
Election for the SAA Committee occurring this month!
On June 4th, SAA Members should have received an e-mail with the invitation to participate in the election of the SAA committee. This year, new EC members will be elected for four positions: President-Elect, Treasurer, Member-at-Large, and the Early Career Member-at-Large.
Please take part in this election and cast your vote by June 24th. The current Executive Committee are very grateful to have received several nominations for the open positions this year and hope for a high voter turnout among the membership. If you have any questions on the procedure, please reach out to the Executive Committee (info[at]ambulatory[dot]assessment[dot]org). Thank you very much for participating in this year’s election.
Notifications and Recognition
Signal Boost: Congratulations to Prof. Eeske van Roekel!

In May 2026, Eeske van Roekel was appointed to Professor in the Department of Developmental Psychology at the Tilburg School of Social and Behavioral Sciences (TSB), Tilburg University. Her research program is focused on the emotional well-being of young people.
With innovative methods, such as real-time measurements via smartphones, she develops personal interventions that support young people when it really matters. Her work thus bridges the gap between science and practice, with an impact on both research and society. Congratulations Prof. van Roekel on this well deserved honor.
Reminder to send a Signal Boost!
We did not receive many “Signal Boost” messages this spring. BUT this does not mean that there were no SAA member accomplishments, assistance, and/or achievements to celebrate. As a reminder, a “Signal Boost” could be winning a award, getting a promotion, defending a thesis/dissertation, obtaining a grant, helping with an analysis, solving a vexing technical problem, or anything else that deserves recognition. Also, don’t be shy and feel free to Signal Boost yourself for an achievement or milestone you would like to share! We would love to hear from more members!

To submit a Signal Boost, follow the instructions below:
- Click the icon on the right
- Enter “Signal Boost” in the subject line
- Clearly identify the SAA member that you would like to recognize and write a brief description of why you would like to recognize this individual.
Community Information
Seeking: Research Coordinator at Palo Alto VA Medical Center-Menlo Park
A Palo Alto Health Care System
Menlo Park, CA 94025
Dr. Haijing Hallenbeck is hiring a full-time research coordinator to assist with a VA-funded study based at the Menlo Park VA campus, ideally starting in October 2026. The study involves building and testing a mobile health intervention to improve symptoms and functioning in Veterans with PTSD and depression. Responsibilities include: recruiting, screening, and scheduling participants; conducting in-person study visits; and managing data and assisting with data analysis and manuscript preparation. On-site work is required. Experience conducting clinical interviews (e.g., SCID-5) is a plus but not required. High attention to detail and strong interpersonal and organizational skills are desired. The research assistant will also support other studies involving mobile health assessments or interventions in a Veteran population. Additionally, they will receive research mentoring and other opportunities for professional development (e.g., presenting at conferences). This position is an ideal fit for aspiring applicants to graduate or medical school looking to gain research experience at the intersection of mental health and technology.
Basic Requirements:
- Must be a U.S. Citizen and authorized to work in the U.S.
- Bachelor’s or Master’s degree in Psychology, Neuroscience, Social Sciences, Public Health, or related field
- At least one year of previous research experience
Job Type: Full-time, W2
Position Duration: Minimum commitment of one year, preferred commitment of three years
Salary Range: $63,081-$77,161, depending on degree (Bachelor’s or Master’s) and experience
To be considered for the position, please email Dr. Hallenbeck at [email protected]with a cover letter and resume/CV, along with contact information for two references. Review of materials will be conducted on a rolling basis until the role is filled.
In memoriam Michael Myrtek (1941-2025)
Michael Myrtek, Professor Emeritus at Freiburg University, Germany, passed away on November 19, 2025. Myrtek was a pioneer of ambulatory psychophysiological assessment and a passionate researcher (and mountain hiker).
He studied Medicine and Psychology at the Albert-Ludwigs University, Freiburg, Germany, where he received his MD in 1967. In 1979, he was appointed Professor for Psychophysiology at Freiburg University.
Together with Jochen Fahrenberg, he led the psychophysiology research lab at Freiburg University. Beginning in 1970, Fahrenberg and Myrtek initiated an impressive research program: The ambitious goal was to establish standardized physiological and psychological assessment protocols to test models grounded in emotion theory, personality psychology, and psychosomatic medicine. Early on, they realized the limits of laboratory research when it came to ecological validity and the generalizability of findings. Hence, they soon expanded their research agenda to include innovative ambulatory measures and protocols.
In the early 1980es, Myrtek and colleagues developed the Freiburg Monitoring System to assess in everyday life the electrocardiogram, physical activity, and the psychological evaluation of the situation. The system immediately analyzed the physiological data and prompted EMA-style self-reports, when an increase in physiological arousal was detected.
Together with Jochen Fahrenberg, Michael Myrtek organized conferences on Ambulatory Assessment and published the state of research in two volumes (1996 “Ambulatory Assessment”, 2001 “Progress in Ambulatory Assessment”), which were among the first comprehensive textbooks in the field. His contribution to Ambulatory Assessment research is lasting.
He will be dearly missed.
Peter Wilhelm
Thomas Kubiak
Ulrich W. Ebner-Priemer
SAA Communication Committee Members
- R. Ross MacLean, Ph.D. (Committee Chair), Yale School of Medicine and VA Connecticut Healthcare System
- Lauren DiPaolo, Ph.D., Corporal Michael J. Crescenz VA Medical Center
- Anne Grünert, Ph.D., RWTH Aachen University
- Haijing Hallenbeck, Ph.D., VA National Center for PTSD and Stanford University Medical Center
- Julia Heckmann-Umhau, M.Sc, Universität Heidelberg
- Laura König, Ph.D., University of Vienna
- Femke Lamers, Ph.D., Amsterdam University Medical Center